
Blog
Twin Health Prediabetes and Healthy Weight Programs Deliver Significant Outcomes and Savings
Oops! This content is hosted in another place.
Find it HereHow Twin’s insight-driven, expert care can prevent the onset and progression of cardiometabolic disease, lowering costs by $7,532 per member over 2 years
Obesity and prediabetes rates are rising faster than traditional healthcare can keep up. Together, they create a growing clinical and economic burden for healthcare providers and payers: more members with higher medication use inclusive of high-cost GLP-1s, more complex claims, and elevated cardiometabolic risks, such as significant likelihood of progression to type 2 diabetes.
That progression is costly. Individuals who move from prediabetes to type 2 diabetes incur approximately $3,600 more in annual healthcare expenditures in the first year after diagnosis than those who do not progress.1 As complications and comorbidities accumulate, the cost burden compounds while diminishing individuals quality of life.
In addition, traditional weight management and prediabetes programs increasingly rely on GLP-1 medications without clinical stewardship — or a clear plan on how patients can get the most out of their GLP-1, manage side effects, get off their regimen, and avoid rebound effects after stopping. This unstewarded treatment drives poor outcomes with open-ended use and compounding costs for employers and health plans.
The need is critical and clear: intervene earlier, personalize care more deeply and more often, and improve the biology and conditions that drive downstream healthcare costs, investing in long-term health. Twin is built for this need — prevention — and our data proves it.
Prevention through proactive, precision care
Twin delivers personalized cardiometabolic care, inclusive of healthy weight and prediabetes programs, through expert clinicians guided by each member’s AI Digital Twin, which along with a direct-to-member engagement tool make up an end-to-end care delivery system: the Digital Twin Care Platform. Fueled by sensor-based monitoring and other real-world data inputs, it’s a level of continuous, individualized insight in biology and behavior traditional care can’t provide.
This is because most medical systems are built around snapshots: office visits, lab results, medication refills, or periodic check-ins. Between those moments, providers have limited visibility into what is changing in a person’s body, habits, medications, and their biological response.
Twin closes those blind spots.
▶️ The Digital Twin Care Platform continuously learns from each member’s biology and behavior, fueled by sensor-based monitoring and wearables.
▶️ This informs Twin care teams on their response to food, activity, sleep, stress, medication, and other daily drivers of cardiometabolic health.
▶️ That insight enables clinicians and coaches to guide timely, personalized care and action, not generic advice or episodic care.
Twin’s Digital Twin translates real-world data into real-time care decisions, making precision care possible in daily life.

Study proof: better outcomes, lower costs with Twin2
In a 24-month study of 302 commercially-insured participants across 8 employer groups, members enrolled in Twin’s prediabetes and healthy weight programs achieved sustained clinical improvements and consequent, measurable savings.
About the study
Study participants were Twin members, both male and female aged 52 (average) with prediabetes or a BMI greater or equal to 30 (an obesity diagnosis). They were followed by the program continuously over two years.
Clinical outcomes were measured via:
- Weight and blood pressure via home connected devices
- Glycemic & cardiometabolic markers — A1C, lipids, kidney and liver function — via quarterly labs
- A1C via wearable CGMs
- GLP-1 use via internal Twin medical records and claims records
Economic analysis was conducted via:
- Baseline costs from BMI + medication use
- Program costs included BMI-adjusted spend, medications, avoided type 2 diabetes, and fees²
- Net savings = program vs. baseline costs program fees using published methods3

Spotlight on preventing type 2 diabetes progression
The study demonstrated meaningful prevention of progression to type 2 diabetes among a high-risk population with prediabetes, obesity, and insulin resistance.
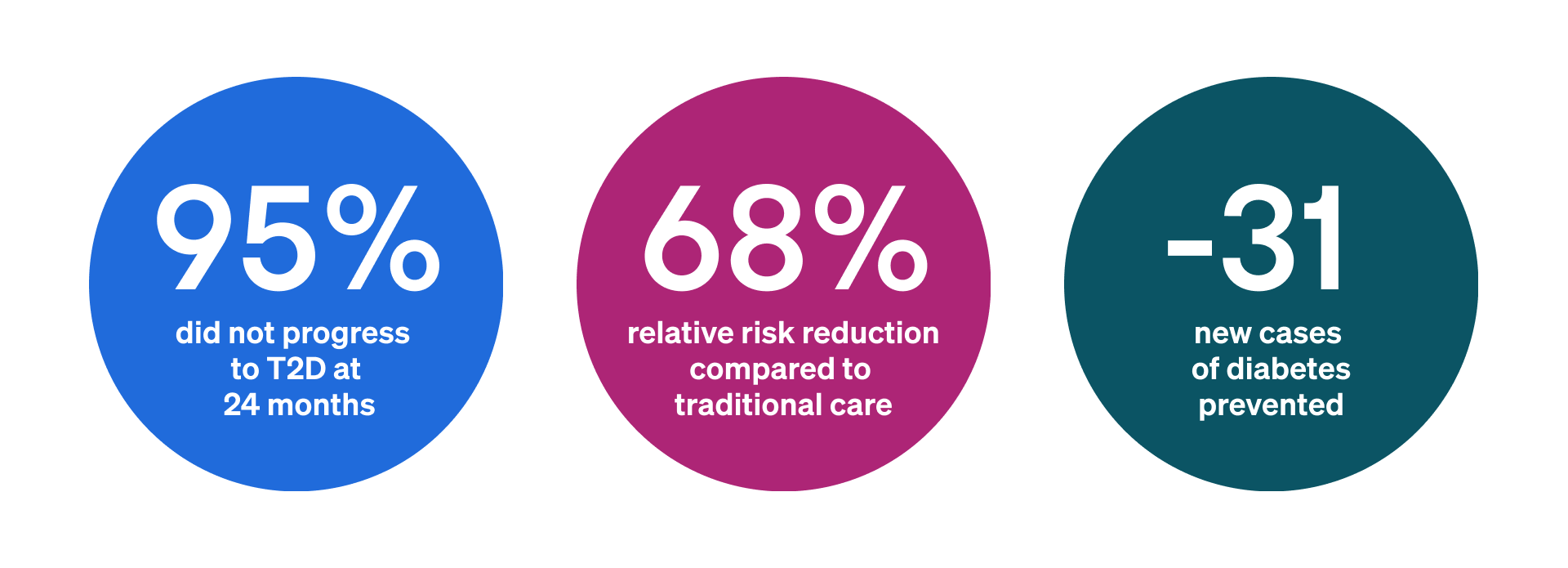
- At 24 months, 95% of participants remained free from progression to type 2 diabetes, compared to a calibrated national benchmark of approximately 8% annual progression for similar high-risk populations.4.5
- That translated to an observed 5% progression rate over two years — an approximately 68% relative risk reduction versus expected progression.
- In total, the program was estimated to prevent 31 new cases of type 2 diabetes, each associated with roughly $3,600 in additional annual healthcare expenditures after diagnosis as stated above.
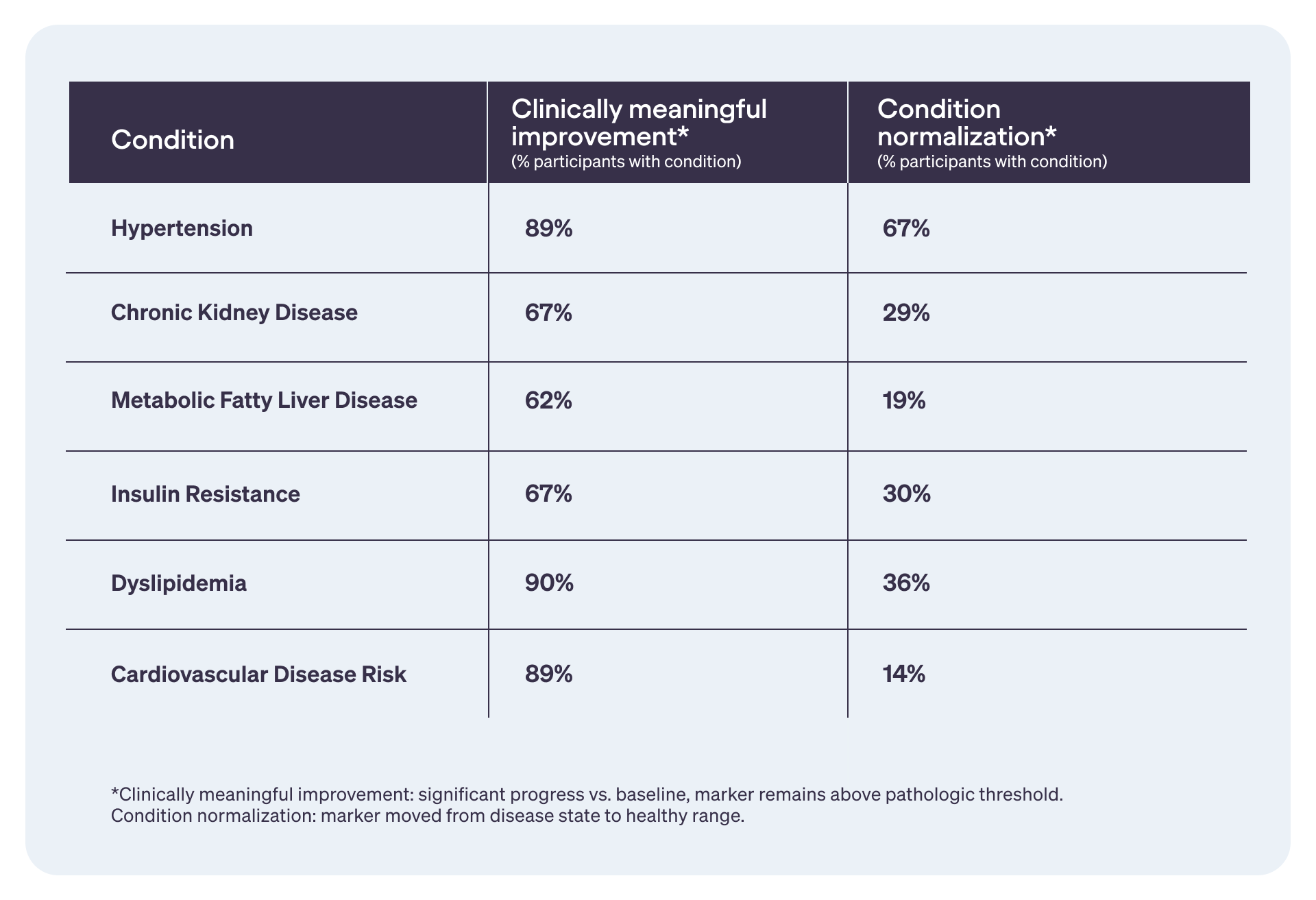
Cardiometabolic healing compounds diabetes risk reduction2
While Twin’s programs focused on weight loss and preventing progression from prediabetes to type 2 diabetes, many participants improved or normalized key markers tied to hypertension, kidney disease, fatty liver disease, insulin resistance, dyslipidemia, and overall cardiovascular risk.
This reinforces Twin’s whole-body approach to care and the one-on-one relationship between biological improvements and lower long-term health risks, ensuring our partners’ investments endure, too.
With Twin, employers can save at least $7,532 per employee over 2 years through weight loss, fewer medications, and clinical improvements, reducing risk of type 2 diabetes.2
Prevention pays in health and savings
Savings reached $2,756 per participant after one year, and $7,532 per participant over two years as largely:
- weight loss was maintained,
- medication dependence declined,
- and expected diabetes progression was avoided.
Yet, these projected savings are meaningful, but also conservative.
They exclude indirect costs such as productivity, absenteeism, presenteeism, and caregiver burden. They also don’t capture the full long-term value of preventing or delaying type 2 diabetes related to avoiding medication escalation, cardiovascular complications, kidney disease, and future high-cost claims.
The participant group also enrolled before broad weight-loss GLP-1 utilization, with lower use at baseline than what we’re observing now. More recently enrolled Twin populations have higher baseline GLP-1 use, meaning medication tapering and discontinuation could become a larger, additive source of savings in future analyses.
Bottom line: the $7,532 figure reflects measurable two-year savings, but not the full lifetime value of preventing metabolic disease progression.
The preventive path to lower total cost of care
Twin helps payers and plan sponsors get ahead of cardiometabolic risk before it worsens, is more expensive, and harder to treat. Through real-time views into member’s biology and behavior, Twin clinicians help members reverse metabolic dysfunction to drive down costly, complex conditions risks — cardiovascular disease, type 2 diabetes, obesity, and others, while reducing dependency on GLP-1s.
Better health. Fewer medications. Less progression. Lower costs.
Learn even more compelling study results, and how Twin’s preventive programs can improve your population’s health while reducing total cost of care.
Connect with us >>
Footer & Sources
A1C = glycosylated hemoglobin; BMI = body mass index; CGM = continuous glucose monitor; GLP-1 = glucagon-like peptide-1 receptor agonists; T2D = type 2 diabetes
- Khan T, Tsipas S, Wozniak G. Medical Care Expenditures for Individuals with Prediabetes: The Potential Cost Savings in Reducing the Risk of Developing Diabetes. Popul Health Manag. 2017;20(5):389–396. doi:10.1089/pop.2016.0134
- Twin Health internal analysis of 302 commercially insured participants across 8 employers enrolled in the Twin Program between 2023–2025; data on file published May, 2026.
- Obesity, Diabetes and CVD Collaboration. The Lancet Global Health. 2025.
- Tabák AG, et al. Prediabetes: a high-risk state for diabetes development. The Lancet. 2012;379(9833):2279–2290. PMCID: PMC3891203
- Centers for Disease Control and Prevention. Prediabetes Statistics. U.S. Department of Health & Human Services; 2024. https://www. cdc.gov/diabetes/communication-resources/prediabetes-statistics.html
No content exists for this entry